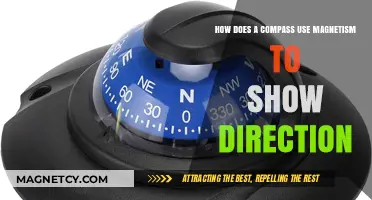
Electroconvulsive Therapy (ECT) and Magnetic Seizure Therapy (MST) are two distinct yet related therapeutic approaches that have been used in the treatment of severe mental health conditions, particularly major depressive disorder and treatment-resistant depression. While both therapies involve inducing controlled seizures to alleviate symptoms, they differ in their methods: ECT uses electrical currents, whereas MST employs magnetic fields. Despite advances in psychiatric medications and other treatments, ECT remains a widely used and effective intervention, especially for severe cases where other treatments have failed. MST, on the other hand, is a newer and less invasive alternative that is still being researched and is not as widely adopted. This raises the question: Are ECT and MST still relevant and utilized in modern psychiatric practice, and how do they compare in terms of efficacy, safety, and patient acceptance?
Explore related products






What You'll Learn
- ECT's Evolution: Modern techniques reduce side effects, making it a viable treatment option today
- Magnetic Seizure Therapy: Non-invasive alternative to ECT, using magnetic fields to induce seizures
- Current Usage Trends: Both therapies are still used for treatment-resistant depression and other disorders
- Effectiveness Comparison: ECT remains more widely used due to its proven efficacy over decades
- Patient Preferences: Some patients prefer magnetic seizure therapy for its fewer cognitive side effects
![]()
ECT's Evolution: Modern techniques reduce side effects, making it a viable treatment option today
Electroconvulsive therapy (ECT) has undergone significant transformations since its inception in the 1930s, evolving from a controversial procedure to a refined, evidence-based treatment. Modern ECT techniques prioritize minimizing side effects while maximizing therapeutic benefits, making it a viable option for severe mental health conditions like treatment-resistant depression, bipolar disorder, and schizophrenia. One key advancement is the use of brief-pulse stimulation, which delivers shorter bursts of electricity (typically 0.5–2.0 millisecond pulses) compared to the earlier sine-wave method. This reduces cognitive side effects, such as memory loss, by targeting specific brain regions more precisely. Additionally, the introduction of unilateral ECT, where electrodes are placed on one side of the head rather than both, further mitigates memory impairment while maintaining efficacy.
Another critical improvement is the standardization of anesthesia and muscle relaxation protocols. Patients now receive general anesthesia and a muscle relaxant to prevent the violent convulsions once associated with ECT. This not only makes the procedure safer but also more comfortable, reducing fear and stigma. For instance, succinylcholine, a short-acting muscle relaxant, is commonly used to induce controlled seizures lasting 30–60 seconds, followed by rapid recovery. These measures have made ECT an outpatient procedure for many, with patients typically returning home the same day after a brief monitoring period.
The advent of personalized treatment plans has also enhanced ECT’s effectiveness. Psychiatrists now tailor the number of sessions, electrode placement, and stimulus intensity based on individual patient profiles, including age, diagnosis, and treatment history. For example, older adults or those with cognitive vulnerabilities may receive lower doses or unilateral ECT to minimize memory-related side effects. Conversely, patients with severe symptoms may require bilateral ECT for more robust results. This individualized approach ensures that the benefits of ECT outweigh its risks for each patient.
Despite these advancements, ECT is not without challenges. Patients and caregivers must be educated about the procedure’s nuances, including potential side effects like headaches, muscle soreness, and temporary confusion. Practical tips, such as arranging transportation post-treatment and scheduling sessions early in the day to allow for rest, can improve the overall experience. Moreover, integrating ECT with psychotherapy and medication management often yields better long-term outcomes, emphasizing its role as part of a comprehensive treatment strategy.
In conclusion, modern ECT is a far cry from its early days, thanks to innovations that prioritize safety, comfort, and efficacy. By reducing side effects and personalizing treatment, it remains a valuable tool for individuals who have not responded to other interventions. As research continues, ECT’s evolution underscores its relevance in contemporary psychiatry, offering hope to those with the most treatment-resistant conditions.
Ancient Chinese Magnet Mastery: Unveiling Early Magnetic Innovations and Uses
You may want to see also
Explore related products






![]()
Magnetic Seizure Therapy: Non-invasive alternative to ECT, using magnetic fields to induce seizures
Electroconvulsive therapy (ECT) has long been a standard treatment for severe depression and other psychiatric disorders, but its side effects, particularly memory loss, have spurred the search for less invasive alternatives. Magnetic seizure therapy (MST) emerges as a promising candidate, leveraging magnetic fields to induce controlled seizures without the need for electrical currents. Unlike ECT, which requires general anesthesia and delivers electricity directly to the brain, MST uses transcranial magnetic stimulation (TMS) technology to target specific brain regions with precision. This non-invasive approach minimizes systemic risks and reduces cognitive side effects, making it an attractive option for patients who are hesitant about traditional ECT.
The procedure for MST involves placing a magnetic coil on the scalp, which delivers rapid, high-intensity pulses to induce a seizure. The duration and frequency of these pulses are carefully calibrated—typically ranging from 20 to 100 Hz—to ensure therapeutic efficacy while avoiding excessive brain stimulation. Patients undergoing MST remain awake during the procedure, and the induced seizure lasts only a few seconds, followed by a brief recovery period. This contrasts sharply with ECT, where patients are under anesthesia and experience longer seizures, often accompanied by post-treatment confusion. MST’s targeted nature allows for more localized treatment, potentially reducing the cognitive impact on memory and executive function.
Clinical trials have shown that MST can be as effective as ECT in treating severe depression, particularly in treatment-resistant cases. A 2021 study published in *Neuropsychopharmacology* reported significant symptom reduction in 60% of patients after a series of MST sessions, with fewer complaints of memory impairment compared to ECT. However, MST is still in the experimental phase, and its long-term efficacy and safety profile are not yet fully established. Researchers are exploring optimal dosing protocols, such as the number of sessions (typically 6–12) and pulse intensity, to maximize benefits while minimizing risks.
One of the key advantages of MST is its potential to treat a broader range of patients, including older adults and those with medical comorbidities who may not tolerate ECT. For instance, individuals with cardiovascular conditions or respiratory issues may find MST a safer alternative due to its non-invasive nature and absence of anesthesia. However, MST is not without limitations. The cost of equipment and the need for specialized training currently restrict its availability to select research centers. Additionally, not all patients respond to MST, and further research is needed to identify predictive biomarkers for treatment success.
In conclusion, magnetic seizure therapy represents a significant advancement in the field of neuromodulation, offering a non-invasive alternative to ECT with reduced cognitive side effects. While still in the experimental stage, its potential to revolutionize treatment for severe depression and other psychiatric disorders is undeniable. As research progresses and technology becomes more accessible, MST could become a mainstream option, providing hope for patients seeking safer and more targeted interventions. For now, clinicians and patients alike await further evidence to guide its integration into standard psychiatric care.
Exploring Navigation: Magnetic Compass Uses and Applications Revealed
You may want to see also
Explore related products






![]()
Current Usage Trends: Both therapies are still used for treatment-resistant depression and other disorders
Electroconvulsive therapy (ECT) and magnetic seizure therapy (MST) remain vital tools in modern psychiatry, particularly for treatment-resistant depression (TRD) and other severe mental health disorders. Despite advances in pharmacotherapy and psychotherapy, a significant subset of patients—estimated at 30-40%—do not achieve remission with standard treatments. For these individuals, ECT and MST offer a lifeline, often providing rapid and robust symptom relief where other interventions fail. ECT, with its decades-long track record, is more widely available and studied, while MST, a newer modality, is gaining traction due to its potential for fewer cognitive side effects. Both therapies are administered under anesthesia, ensuring patient comfort, and are tailored to individual needs, with parameters like electrode placement (for ECT) or magnetic coil positioning (for MST) adjusted for optimal outcomes.
Consider the case of a 45-year-old patient with severe TRD who failed to respond to multiple antidepressants and psychotherapy. After a course of 6–12 ECT sessions, administered two to three times weekly, they experienced a 70% reduction in depressive symptoms, as measured by the Hamilton Depression Rating Scale. This example underscores ECT’s efficacy, particularly its ability to act swiftly in acute cases. MST, though less studied, shows promise in preliminary trials, with one study reporting a 50% response rate in TRD patients after 20 sessions. Unlike ECT, MST uses magnetic fields to induce seizures, which may reduce memory impairment—a common concern with ECT. However, MST’s limited availability and higher cost currently restrict its use to specialized centers.
When deciding between ECT and MST, clinicians weigh factors like patient history, cognitive concerns, and treatment urgency. ECT remains the gold standard for severe, life-threatening depression due to its proven efficacy and widespread accessibility. MST, while not yet a first-line option, is increasingly considered for patients with a history of cognitive side effects from ECT or those at high risk for memory loss. For instance, older adults or professionals reliant on sharp memory may benefit from MST’s more targeted approach. Practical tips for patients include maintaining open communication with their care team, tracking mood changes during treatment, and planning for post-treatment support, such as gradual resumption of daily activities.
A comparative analysis reveals that while ECT’s efficacy is well-established, MST’s role is evolving. ECT’s side effects, primarily short-term confusion and memory loss, are well-documented but often transient. MST’s cognitive profile appears more favorable, though larger, long-term studies are needed to confirm its advantages. Both therapies require careful monitoring, including pre-treatment evaluations (e.g., EEG, bloodwork) and post-treatment follow-up to assess response and adjust dosage. For instance, ECT dosage is often titrated based on seizure duration, with a target of 25–40 seconds to balance efficacy and side effects. MST’s parameters, such as magnetic pulse intensity, are similarly fine-tuned to individual tolerance and response.
In conclusion, ECT and MST are not relics of the past but dynamic, evidence-based treatments for TRD and other disorders. Their continued use reflects psychiatry’s commitment to addressing unmet needs in mental healthcare. While ECT remains the more established option, MST’s emergence offers hope for a future with fewer cognitive trade-offs. Patients and providers alike must stay informed about these therapies’ evolving roles, ensuring that those with treatment-resistant conditions receive the most effective and personalized care possible.
Magnetic Marvels: How Bullet Trains Use Magnets for Speed
You may want to see also
Explore related products






![]()
Effectiveness Comparison: ECT remains more widely used due to its proven efficacy over decades
Electroconvulsive therapy (ECT) has stood the test of time, remaining a cornerstone in the treatment of severe mental health disorders, particularly major depressive disorder and bipolar disorder. Its enduring use is rooted in decades of clinical evidence demonstrating significant efficacy, often where other treatments fail. For instance, ECT achieves remission rates of 70–90% in treatment-resistant depression, a stark contrast to the 30–40% success rate of most antidepressant medications. This proven track record ensures its continued preference among clinicians, especially in urgent cases like suicidal ideation or severe psychosis.
Magnetic seizure therapy (MST), while innovative, has yet to match ECT’s established effectiveness. MST uses magnetic fields to induce seizures in a more localized brain region, theoretically reducing cognitive side effects. However, current studies show MST’s remission rates for depression hover around 30–50%, significantly lower than ECT. Additionally, MST’s optimal dosage and frequency remain under investigation, with protocols varying widely across trials. For example, some studies use 10–20 sessions at 100–120% of motor threshold, while others experiment with fewer sessions at higher intensities. This lack of standardization limits its widespread adoption.
The comparative advantage of ECT extends beyond efficacy to its versatility. It is approved for use across a broad age range, from adolescents to the elderly, with adjustments made for factors like age and comorbidities. For instance, elderly patients often receive lower electrical dosages (e.g., 25–50% of the standard dose) to minimize risks. In contrast, MST’s safety profile in diverse populations remains under-researched, particularly in vulnerable groups like pregnant women or those with neurological conditions. This gap in data further cements ECT’s dominance in clinical practice.
Practically, ECT’s integration into treatment protocols is well-established, with clear guidelines for administration, anesthesia, and post-treatment care. For example, bilateral ECT (targeting both brain hemispheres) is often preferred for rapid symptom relief, while unilateral ECT (one hemisphere) is chosen to minimize memory impairment. MST, despite its theoretical advantages, lacks such standardized protocols, leaving clinicians hesitant to adopt it as a first-line option. Until MST’s efficacy and safety data rival ECT’s, the latter will remain the gold standard for severe, refractory mental health conditions.
Exploring Magnetic Resonance Imaging: Uses and Applications in Modern Medicine
You may want to see also
Explore related products






![]()
Patient Preferences: Some patients prefer magnetic seizure therapy for its fewer cognitive side effects
Electroconvulsive therapy (ECT) and magnetic seizure therapy (MST) remain viable treatments for severe mental health conditions, but patient preferences increasingly tilt toward MST due to its reduced cognitive side effects. Unlike ECT, which uses electrical currents to induce seizures, MST employs magnetic fields to target specific brain regions, minimizing memory loss and confusion. For patients weighing treatment options, this distinction is critical. For instance, a 45-year-old professional with treatment-resistant depression might opt for MST to avoid the weeks of cognitive impairment often associated with ECT, which can disrupt work and daily functioning.
The preference for MST is rooted in its precision and gentler impact on cognitive function. Studies show that MST patients report fewer instances of retrograde amnesia—the inability to recall past events—compared to ECT recipients. This is particularly appealing for older adults or individuals with memory-intensive careers. However, MST’s effectiveness is still being refined, and it may require more sessions than ECT to achieve comparable results. For example, while ECT typically involves 6–12 sessions, MST protocols often extend to 15–20 sessions, each lasting about 30 minutes.
Clinicians must balance patient preferences with clinical efficacy when recommending MST. While its cognitive advantages are clear, MST’s availability is limited due to high equipment costs and specialized training requirements. Patients considering MST should inquire about facility accreditation and practitioner experience, as improper administration can reduce efficacy or increase risks. Additionally, combining MST with psychotherapy or medication can enhance outcomes, particularly for conditions like severe depression or bipolar disorder.
Practical considerations also play a role in patient choice. MST sessions are generally outpatient procedures, allowing individuals to return home the same day. Post-treatment, patients are advised to avoid driving for 24 hours and to monitor for mild side effects like headaches or scalp discomfort. In contrast, ECT often requires anesthesia and a longer recovery period, which may deter those seeking less invasive options. Ultimately, the decision between ECT and MST hinges on individual priorities: rapid symptom relief versus cognitive preservation. For many, MST’s promise of clearer thinking post-treatment makes it the preferred choice.
Securely Erase Data: Using Magnets to Destroy Hard Drives Safely
You may want to see also
Frequently asked questions
Yes, both ECT and MST are still used today, particularly for severe and treatment-resistant mental health conditions like major depression, bipolar disorder, and schizophrenia.
ECT and MST are primarily used for severe depression, especially when other treatments like medication and therapy have failed. They are also used in cases of severe mania, catatonia, and certain psychotic disorders.
ECT involves delivering an electrical current to the brain to induce a controlled seizure, while MST uses magnetic fields to achieve the same effect. MST is generally associated with fewer cognitive side effects, such as memory loss, compared to ECT.
Both treatments are considered safe when administered by trained professionals. Good candidates include individuals with severe, life-threatening mental health conditions who have not responded to other treatments. However, a thorough evaluation by a psychiatrist is necessary to determine suitability.