Transcranial Magnetic Stimulation (TMS) is a non-invasive brain stimulation technique that uses magnetic fields to modulate neural activity in specific regions of the brain. It involves placing a magnetic coil against the scalp, which delivers brief, targeted pulses to stimulate or inhibit underlying brain cells. TMS is widely used in both clinical and research settings, particularly for treating conditions like depression, anxiety, and chronic pain, as well as for studying brain function and connectivity. Understanding how to use TMS effectively requires knowledge of proper coil placement, stimulation parameters, and safety protocols to ensure optimal outcomes and minimize risks. This technique has gained popularity due to its precision, lack of systemic side effects, and potential to offer relief for patients who have not responded to traditional treatments.
Explore related products






What You'll Learn
- TMS Basics: Understand TMS device, coil placement, and stimulation parameters for effective treatment
- Safety Protocols: Learn contraindications, side effects, and patient screening for safe TMS application
- Targeted Brain Regions: Identify areas like DLPFC for depression or motor cortex for movement
- Session Procedures: Follow step-by-step protocols for setup, stimulation, and post-session care
- Clinical Applications: Explore TMS uses for depression, anxiety, pain, and neurological disorders
![]()
TMS Basics: Understand TMS device, coil placement, and stimulation parameters for effective treatment
Transcranial Magnetic Stimulation (TMS) devices are the cornerstone of this non-invasive brain stimulation technique, and understanding their mechanics is crucial for effective treatment. These devices generate brief magnetic pulses via a coil placed on the scalp, inducing electrical currents in targeted brain regions. The core component is the stimulator, which controls pulse intensity, frequency, and duration. Modern TMS machines, such as the MagPro X100 or NeuroStar, offer precision and user-friendly interfaces, ensuring consistent delivery of therapeutic stimulation. The magnetic field strength, typically measured in Tesla (T), determines penetration depth and neural activation, with most devices operating between 1.5 to 2.0 T. Selecting the right device is the first step in tailoring TMS to individual patient needs.
Coil placement is a critical factor in TMS efficacy, as it determines which brain regions are stimulated. The most common coil type is the figure-of-eight coil, ideal for targeting focal areas like the dorsolateral prefrontal cortex (DLPFC), a key site for treating depression. Placement is guided by anatomical landmarks, such as the F3/F4 positions in the EEG 10-20 system, or by neuronavigation systems for greater accuracy. For instance, the coil should be positioned 5 cm anterior to the motor cortex to target the DLPFC effectively. Improper placement can lead to suboptimal outcomes or unintended stimulation of adjacent areas. Practitioners often use structural MRI scans to ensure precise localization, especially in patients with atypical brain anatomy.
Stimulation parameters—frequency, intensity, and train duration—dictate the therapeutic effect of TMS. Low-frequency stimulation (≤1 Hz) typically inhibits neural activity, while high-frequency stimulation (≥5 Hz) excites it. For depression, high-frequency TMS (10–20 Hz) over the left DLPFC is standard, with sessions lasting 20–40 minutes. Intensity is often set at 80–120% of the patient’s resting motor threshold (RMT), the minimum stimulation required to induce a motor response in the hand. Protocols vary; for example, the Theta Burst Stimulation (TBS) method uses shorter, patterned bursts for quicker sessions. Adjusting these parameters based on patient response and tolerance is essential for optimizing outcomes.
Practical considerations and safety precautions are paramount in TMS administration. Patients should be screened for contraindications, such as metallic implants or a history of seizures. Side effects are generally mild, including scalp discomfort or headaches, but rare cases of induced seizures highlight the need for adherence to safety guidelines. Sessions are typically conducted daily, Monday through Friday, for 4–6 weeks, though maintenance protocols may extend treatment. Clinicians must monitor patients closely, adjusting parameters as needed to balance efficacy and comfort. With proper technique and attention to detail, TMS offers a promising, evidence-based approach to treating neurological and psychiatric disorders.
Mastering Keyless Entry: Schlage Magnetic Door Lock Installation Guide
You may want to see also
Explore related products






![]()
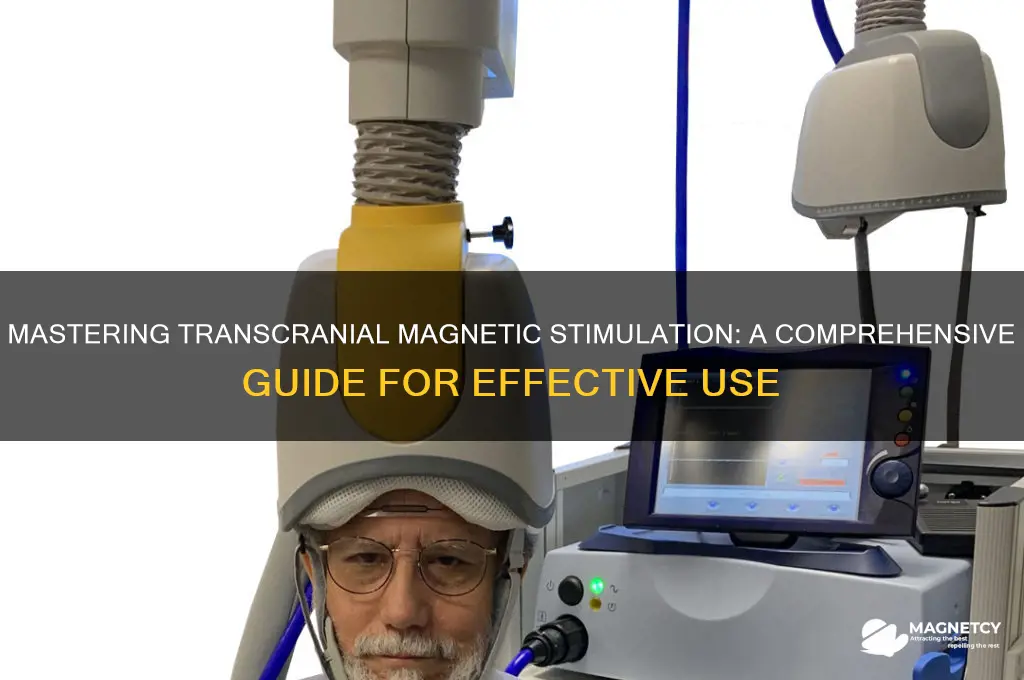
Safety Protocols: Learn contraindications, side effects, and patient screening for safe TMS application
Transcranial Magnetic Stimulation (TMS) is a powerful tool in neuroscience and clinical practice, but its safe application hinges on rigorous adherence to safety protocols. Before initiating treatment, clinicians must thoroughly understand contraindications, potential side effects, and patient screening procedures to mitigate risks and ensure optimal outcomes.
Contraindications serve as the first line of defense in TMS safety. Absolute contraindications include the presence of ferromagnetic materials in the head or neck, such as aneurysm clips or cochlear implants, which can heat up or move under the magnetic field. Relative contraindications, like a history of seizures or severe migraines, require careful consideration and often necessitate consultation with a neurologist. For instance, patients with a seizure threshold lowered by medications or pre-existing conditions may face increased risks, even at standard stimulation intensities (typically 110-120% of motor threshold). Pediatric and geriatric populations also demand special attention; TMS is generally not recommended for children under 12 due to incomplete brain development, while elderly patients may require lower stimulation intensities to account for age-related neural changes.
Side effects, though usually mild and transient, must be monitored and managed. The most common side effect is scalp discomfort or pain at the stimulation site, reported by up to 50% of patients. Less frequently, TMS can induce headaches, lightheadedness, or facial twitching. Rarely, seizures occur, with an estimated incidence of 0.03% in clinical settings. To minimize these risks, clinicians should start with lower stimulation intensities and gradually titrate upward, ensuring patient tolerance. For example, a protocol might begin at 80% of the estimated motor threshold and increase by 5% increments until therapeutic levels are reached. Patients should be educated about potential side effects and instructed to report any unusual symptoms immediately.
Patient screening is a critical step that cannot be overlooked. A comprehensive evaluation should include a detailed medical history, neurological examination, and psychiatric assessment. Key questions to ask include inquiries about metal implants, seizure history, and current medications, as certain drugs (e.g., antidepressants, antipsychotics) may alter cortical excitability. Practical tips for screening include using standardized checklists to ensure consistency and involving a multidisciplinary team when complex cases arise. For instance, a patient with a history of traumatic brain injury might require additional imaging to rule out subtle metallic fragments before proceeding with TMS.
In conclusion, mastering safety protocols is essential for the responsible use of TMS. By rigorously identifying contraindications, proactively managing side effects, and conducting thorough patient screenings, clinicians can harness the therapeutic potential of TMS while safeguarding patient well-being. This meticulous approach not only minimizes risks but also fosters trust and confidence in this innovative treatment modality.
Unlocking Magnet Power: Practical Uses in Everyday Life and Beyond
You may want to see also
Explore related products






![]()
Targeted Brain Regions: Identify areas like DLPFC for depression or motor cortex for movement
Transcranial Magnetic Stimulation (TMS) is a non-invasive technique that relies on precise targeting of brain regions to achieve therapeutic effects. The key to its success lies in identifying the specific areas associated with the condition being treated. For instance, the dorsolateral prefrontal cortex (DLPFC) is a primary target for depression, while the motor cortex is crucial for movement-related interventions. Understanding these regions and their roles is essential for effective TMS application.
Analytical Perspective: The DLPFC, located in the frontal lobe, plays a significant role in mood regulation and cognitive control. Studies have shown that stimulating this area at a frequency of 10-20 Hz, with an intensity of 110-120% of the motor threshold, can alleviate symptoms of major depressive disorder. This targeted approach is particularly beneficial for treatment-resistant patients, offering a viable alternative to traditional antidepressants. In contrast, the motor cortex, situated in the frontal lobe near the central sulcus, is responsible for initiating voluntary movements. Stimulating this region at lower frequencies (1-5 Hz) can modulate neural activity, making it a valuable target for conditions like stroke rehabilitation or Parkinson’s disease.
Instructive Approach: To target the DLPFC for depression, position the TMS coil at the F3 or F4 location according to the 10-20 EEG system, approximately 5 cm anterior to the motor cortex. Ensure the coil is angled at 45 degrees to the sagittal plane to maximize focal stimulation. For motor cortex stimulation, place the coil directly over the hand or leg area, identified by mapping motor evoked potentials (MEPs). Begin with a lower intensity (e.g., 80% of resting motor threshold) and gradually increase to the desired level, typically 110-120% for depression or 90-100% for movement disorders. Sessions usually last 20-30 minutes, with treatments administered daily for 4-6 weeks.
Comparative Insight: While both the DLPFC and motor cortex are frequently targeted in TMS, their applications differ significantly. The DLPFC is primarily used for psychiatric conditions, such as depression and anxiety, where emotional and cognitive processes are impaired. In contrast, the motor cortex is targeted for neurological disorders affecting movement, such as stroke or multiple sclerosis. This distinction highlights the importance of tailoring TMS protocols to the specific brain region and condition, ensuring optimal outcomes. For example, a patient with post-stroke hemiparesis would benefit from motor cortex stimulation, whereas someone with treatment-resistant depression would require DLPFC targeting.
Practical Tips: When targeting the DLPFC, consider using neuronavigation systems to enhance precision, especially in patients with anatomical variations. For motor cortex stimulation, ensure the patient is relaxed to avoid muscle contractions that could interfere with MEP recordings. Monitor for side effects such as headaches or scalp discomfort, which are typically mild and transient. For older adults or patients with cognitive impairments, simplify instructions and allow extra time for setup. Always adhere to safety guidelines, such as avoiding TMS in individuals with metallic implants or a history of seizures. By combining technical precision with patient-centered care, TMS can be a powerful tool for targeted brain modulation.
Magnetic Data Storage: How Magnets Preserve Digital Information in Computers
You may want to see also
Explore related products






![]()
Session Procedures: Follow step-by-step protocols for setup, stimulation, and post-session care
Transcranial Magnetic Stimulation (TMS) sessions demand precision and adherence to protocols to ensure safety and efficacy. The setup phase begins with patient positioning, where the individual sits comfortably in a reclined chair, ensuring their head remains stable throughout the procedure. The technician then identifies the target area, typically the dorsolateral prefrontal cortex, using anatomical landmarks or neuroimaging guidance. The TMS coil is positioned over this area, with its orientation adjusted to achieve the desired current direction in the brain. For instance, a figure-eight coil is often angled at 45 degrees to the sagittal plane to induce optimal stimulation. This initial setup is critical, as improper placement can reduce treatment effectiveness or lead to discomfort.
Once the coil is positioned, stimulation parameters are set based on the patient’s motor threshold, which is determined by observing finger twitches in response to varying magnetic pulse intensities. Typically, the stimulation intensity is set at 80%–120% of the motor threshold, with frequencies ranging from 1 Hz for inhibitory effects to 10–20 Hz for excitatory effects. Protocols like theta-burst stimulation (TBS) use patterned bursts of pulses at specific intervals, often administered in sessions lasting 3–20 minutes. During stimulation, patients may hear clicking sounds and feel tapping on the scalp, which is normal. Technicians must monitor for adverse reactions, such as headaches or scalp discomfort, and adjust parameters accordingly.
Post-session care is equally vital to ensure patient comfort and treatment continuity. Patients are advised to avoid strenuous activities for a few hours post-TMS, as mild fatigue or localized discomfort may occur. Hydration and light relaxation techniques, such as deep breathing, can alleviate minor side effects. For individuals undergoing repetitive TMS (rTMS) protocols, consistent attendance is crucial, as missed sessions can disrupt therapeutic progress. Technicians should provide clear instructions on managing any lingering sensations and encourage patients to report persistent symptoms promptly.
Comparatively, TMS procedures differ significantly from other neuromodulation techniques like electroconvulsive therapy (ECT), which requires anesthesia and induces seizures. TMS is non-invasive, requires no sedation, and allows patients to resume daily activities immediately after sessions. However, its success hinges on strict adherence to protocols, from precise coil placement to tailored stimulation parameters. For example, older adults or patients with neurological conditions may require lower intensities or modified frequencies to minimize risks.
In conclusion, mastering TMS session procedures involves a blend of technical precision and patient-centered care. From meticulous setup to vigilant monitoring during stimulation and thoughtful post-session guidance, each step contributes to the treatment’s overall efficacy. By following these protocols, practitioners can maximize therapeutic outcomes while ensuring patient safety and comfort, making TMS a valuable tool in modern neuroscience and mental health care.
Mastering the Magnetic Deep Fryer: Tips for Perfect Crispy Results
You may want to see also
Explore related products






![]()
Clinical Applications: Explore TMS uses for depression, anxiety, pain, and neurological disorders
Transcranial Magnetic Stimulation (TMS) has emerged as a versatile tool in clinical settings, offering non-invasive treatment options for a range of conditions. For depression, TMS is often prescribed when traditional antidepressants fail. The standard protocol involves delivering magnetic pulses to the left dorsolateral prefrontal cortex, a brain region associated with mood regulation. Typically, patients undergo 20–30 sessions, each lasting 20–40 minutes, over 4–6 weeks. The intensity of stimulation is tailored to individual motor thresholds, usually ranging from 80% to 120% of the resting motor threshold. Studies show that approximately 50–60% of treatment-resistant depression patients experience significant improvement, with remission rates around 30%. Practical tips include maintaining consistent session attendance and combining TMS with psychotherapy for enhanced outcomes.
In contrast to depression, TMS for anxiety disorders targets different brain regions, such as the right dorsolateral prefrontal cortex or the anterior cingulate cortex, depending on the specific disorder. For generalized anxiety disorder, low-frequency stimulation (1 Hz) is often used to downregulate hyperactive neural circuits. Protocols vary, but sessions typically last 20–30 minutes, with 10–20 treatments over 2–4 weeks. While research is still evolving, early studies suggest TMS can reduce anxiety symptoms by 20–40%. Patients should be aware that results may take several weeks to manifest, and combining TMS with cognitive-behavioral therapy can amplify benefits.
TMS also shows promise in pain management, particularly for chronic conditions like fibromyalgia and neuropathic pain. High-frequency stimulation (10–20 Hz) is applied to the primary motor cortex or the dorsolateral prefrontal cortex, modulating pain perception pathways. Treatment regimens often consist of 10–15 sessions, each lasting 15–20 minutes. A notable advantage is its minimal side effects compared to opioids or invasive procedures. Patients with pain disorders should consult with a pain specialist to determine the optimal target area and frequency, as these can vary based on the pain’s origin and severity.
For neurological disorders such as Parkinson’s disease, stroke, and multiple sclerosis, TMS is used to enhance neuroplasticity and restore impaired functions. In stroke rehabilitation, low-frequency stimulation is applied to the unaffected hemisphere, while high-frequency stimulation targets the affected hemisphere to promote recovery. Protocols typically involve 10–20 sessions, with each session lasting 10–20 minutes. For Parkinson’s, TMS is often directed at the supplementary motor area to improve motor symptoms. While results are promising, consistency in treatment and patient-specific adjustments are critical. Caregivers should ensure patients are comfortable during sessions, as discomfort can reduce compliance.
Across these applications, TMS stands out for its precision and adaptability. However, it’s essential to note that not all patients respond equally, and individual factors like age, severity of the condition, and comorbidities play a role. Clinicians should carefully assess patients before initiating treatment, and patients should manage expectations, understanding that TMS is a complementary therapy rather than a cure-all. With ongoing research, TMS continues to expand its clinical utility, offering hope to those with limited treatment options.
Effective Terro Fly Magnet Usage: A Step-by-Step Guide to Pest Control
You may want to see also
Frequently asked questions
TMS is a non-invasive brain stimulation technique that uses magnetic fields to stimulate specific areas of the brain. It works by delivering electromagnetic pulses through a coil placed on the scalp, which modulates neural activity in targeted brain regions, often used to treat conditions like depression, anxiety, and other neurological disorders.
TMS is generally not painful, though some individuals may experience mild discomfort, such as a tapping sensation on the scalp or headaches. Common side effects include scalp pain, mild headaches, or lightheadedness, which are usually temporary and resolve on their own.
A typical TMS session lasts about 20–40 minutes, depending on the protocol. Most treatment plans require sessions 5 days a week for 4–6 weeks, totaling around 20–30 sessions. However, the exact number varies based on individual needs and response to treatment.
TMS is often recommended for individuals with treatment-resistant depression or other conditions that haven’t responded to medication or therapy. However, it is contraindicated for people with metal implants in the head (e.g., pacemakers, cochlear implants), a history of seizures, or certain neurological conditions. Always consult a healthcare provider to determine eligibility.