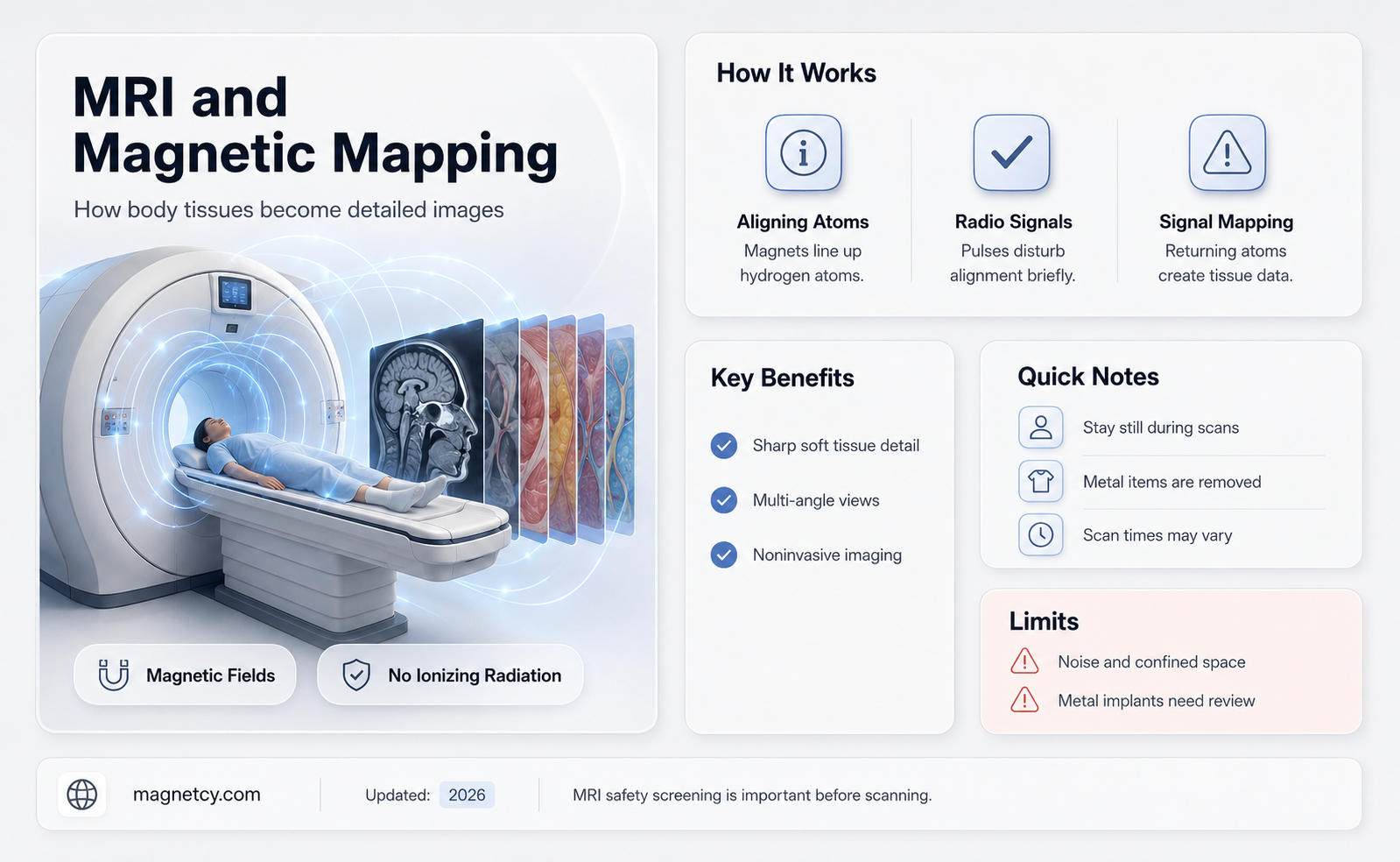
Magnetic resonance imaging (MRI) is a non-invasive medical imaging technique that utilizes powerful magnets and radio waves to generate detailed images of the body’s internal structures. Central to this process are contrast agents, which are substances introduced into the body to enhance the visibility of specific tissues or organs during imaging. These agents work by altering the magnetic properties of tissues, allowing MRI scans to produce clearer, more precise images. Commonly used contrast agents, such as gadolinium-based compounds, are particularly effective in mapping body tissues by highlighting areas of interest, such as blood vessels, tumors, or inflammation, thereby aiding in the diagnosis and monitoring of various medical conditions.
| Characteristics | Values |
|---|---|
| Technology | Magnetic Resonance Imaging (MRI) |
| Primary Purpose | To map and visualize body tissues with high contrast and detail |
| Key Components | Strong magnetic field, radiofrequency coils, gradient coils, computer processing |
| Magnetic Field Strength | Typically 1.5 to 3 Tesla (clinical MRI), up to 7 Tesla (research MRI) |
| Contrast Mechanism | Based on differences in proton density, T1, T2, and T2* relaxation times |
| Tissue Mapping | Differentiates between soft tissues, fat, water, and pathological changes |
| Spatial Resolution | Sub-millimeter to millimeter range |
| Temporal Resolution | Seconds to minutes per image, depending on sequence |
| Safety | Non-invasive, no ionizing radiation, but contraindicated for some implants |
| Applications | Neurology, oncology, cardiology, orthopedics, and more |
| Advantages | High soft-tissue contrast, multiplanar imaging, no radiation exposure |
| Limitations | High cost, long scan times, sensitivity to motion artifacts |
| Common Sequences | T1-weighted, T2-weighted, FLAIR, DWI, SWI |
| Data Output | Cross-sectional images, 3D reconstructions, functional maps (fMRI) |
| Recent Advances | Ultra-high field MRI, AI-assisted image analysis, faster scan techniques |
Explore related products






What You'll Learn
- Contrast Agents: Enhance visibility of specific tissues or organs in MRI scans
- Tissue Relaxation Times: T1, T2, and T2* properties differentiate tissue types
- Diffusion Weighted Imaging: Measures water molecule movement to assess tissue integrity
- Perfusion Imaging: Maps blood flow dynamics in tissues for functional analysis
- Magnetization Transfer: Highlights macromolecular tissue components for detailed contrast
![]()
Contrast Agents: Enhance visibility of specific tissues or organs in MRI scans
Contrast agents are indispensable tools in magnetic resonance imaging (MRI), designed to improve the visibility of specific tissues or organs by altering their signal intensity. These agents, typically gadolinium-based, work by shortening the relaxation times of protons in tissues, thereby enhancing contrast in the resulting images. For instance, in a standard MRI, certain structures like blood vessels or tumors may appear indistinct. Administering a contrast agent can make these areas stand out, allowing radiologists to detect abnormalities with greater precision. This is particularly crucial in diagnosing conditions such as cancer, multiple sclerosis, or cardiovascular diseases, where subtle tissue changes can be indicative of pathology.
The administration of contrast agents follows a precise protocol to ensure safety and efficacy. Typically, gadolinium-based agents are injected intravenously at a dose of 0.1 to 0.2 mmol/kg of body weight, depending on the specific agent and clinical indication. For pediatric patients, dosages are carefully adjusted based on age and weight to minimize risks. It’s essential to monitor patients for adverse reactions, such as allergic responses or nephrogenic systemic fibrosis in those with impaired kidney function. Practical tips include hydrating patients adequately before and after the procedure to facilitate rapid excretion of the contrast agent, particularly in at-risk populations.
Comparatively, contrast-enhanced MRI offers distinct advantages over non-contrast studies, especially in complex cases. For example, in evaluating brain lesions, contrast agents can differentiate between active inflammation and scar tissue, a distinction often impossible without enhancement. Similarly, in abdominal imaging, contrast agents highlight vascular structures and organ perfusion, aiding in the detection of liver tumors or kidney abnormalities. However, the decision to use contrast must weigh benefits against risks, particularly in patients with renal insufficiency or a history of gadolinium reactions. Alternative techniques, such as using higher field strength MRI or advanced sequences, may sometimes suffice, but contrast remains unparalleled in many scenarios.
From a persuasive standpoint, the use of contrast agents in MRI is not merely an option but a necessity in modern diagnostic imaging. Their ability to provide detailed, high-resolution images of internal structures transforms the diagnostic process, enabling earlier and more accurate detection of diseases. For instance, in breast MRI, contrast agents improve sensitivity for detecting malignancies, particularly in dense breast tissue where mammography may fall short. While concerns about gadolinium retention in the body have been raised, studies show that the benefits of contrast-enhanced MRI far outweigh the minimal risks when used judiciously. Radiologists and clinicians must advocate for their appropriate use to maximize patient outcomes.
In conclusion, contrast agents are a cornerstone of MRI, offering unparalleled enhancement of tissue visibility and diagnostic accuracy. Their application requires careful consideration of dosage, patient-specific risks, and clinical context, but when used appropriately, they provide critical insights into tissue pathology. As technology advances, ongoing research into safer, more effective contrast agents promises to further elevate the role of MRI in medical imaging. For practitioners, understanding the nuances of contrast-enhanced MRI is essential to harnessing its full potential in patient care.
Magnets and Kidney Health: Exploring Their Potential Benefits and Risks
You may want to see also
Explore related products






![]()
Tissue Relaxation Times: T1, T2, and T2* properties differentiate tissue types
Magnetic resonance imaging (MRI) leverages the unique relaxation properties of tissues—specifically T1, T2, and T2*—to create detailed anatomical maps. These properties, measured in milliseconds, reflect how quickly hydrogen nuclei return to equilibrium after being disturbed by radiofrequency pulses. T1 (spin-lattice relaxation) represents the recovery of longitudinal magnetization, while T2 (spin-spin relaxation) describes the decay of transverse magnetization. T2*, a variant of T2, accounts for additional signal loss from magnetic field inhomogeneities. Each tissue type exhibits distinct T1, T2, and T2* values, allowing MRI to differentiate between fat, water, muscle, and other structures with remarkable precision.
Consider a practical example: cerebrospinal fluid (CSF) has a long T1 (around 4,000 ms) and a long T2 (around 2,000 ms), making it appear dark on T1-weighted images and bright on T2-weighted images. In contrast, fat has a short T1 (200–300 ms) and a long T2 (80–120 ms), appearing bright on T1-weighted images and moderately bright on T2-weighted images. These differences enable radiologists to identify abnormalities, such as edema (which prolongs T2) or hemorrhage (which shortens T2*). By adjusting MRI sequences to emphasize T1, T2, or T2* properties, clinicians can tailor scans to highlight specific tissue characteristics, improving diagnostic accuracy.
To optimize MRI for tissue differentiation, technicians must carefully select imaging parameters. For instance, a short repetition time (TR) and echo time (TE) enhance T1 contrast, while a long TE maximizes T2 contrast. T2*-weighted imaging, often used in functional MRI and hemorrhage detection, requires minimal TE to capture rapid signal decay. Patients with metallic implants or claustrophobia may require adjustments, such as using shorter sequences or open MRI systems, to ensure accurate results. Understanding these relaxation times empowers both technicians and radiologists to design protocols that reveal subtle tissue variations, from early-stage tumors to degenerative diseases.
A comparative analysis of T1, T2, and T2* reveals their complementary roles in tissue characterization. While T1 and T2 provide stable, intrinsic properties, T2* is more sensitive to external factors like magnetic susceptibility. For example, deoxygenated blood in veins shortens T2* due to local field distortions, creating flow voids in images. This sensitivity makes T2* invaluable for detecting microbleeds or assessing blood oxygenation levels. However, its variability requires careful interpretation to avoid misdiagnosis. By integrating T1, T2, and T2* data, MRI achieves a multidimensional view of tissues, transforming raw signals into clinically actionable insights.
In practice, mastering tissue relaxation times requires a blend of technical skill and clinical knowledge. Radiologists must correlate MRI findings with patient history and other imaging modalities to avoid pitfalls like mistaking artifact for pathology. For instance, a T2* sequence might reveal signal dropout in a patient’s liver, suggesting iron overload, but confirmation via lab tests is essential. Similarly, pediatric scans demand age-specific protocols, as T1 and T2 values evolve with development. By staying attuned to these nuances, healthcare providers can harness the full potential of tissue relaxation properties, turning MRI into a dynamic tool for precision medicine.
Magnetic Marvels: How Bullet Trains Use Magnets for Speed
You may want to see also
Explore related products

$88.99 $98.99





![]()
Diffusion Weighted Imaging: Measures water molecule movement to assess tissue integrity
Water molecules are in constant motion, diffusing through tissues in a pattern influenced by the microstructural environment. Diffusion Weighted Imaging (DWI) harnesses this natural phenomenon, using magnetic resonance principles to measure the random movement of water molecules. By applying specific magnetic field gradients, DWI sensitizes the MRI signal to this diffusion, creating images that reflect the degree of water mobility within tissues. This technique provides a unique window into tissue integrity, as restrictions to water movement—such as those caused by cell membranes, organelles, or pathological changes—alter the diffusion pattern.
The clinical utility of DWI lies in its ability to detect abnormalities at a microscopic level before they become visible on conventional MRI. For instance, in acute ischemic stroke, DWI can identify restricted diffusion in brain tissue within minutes of symptom onset, allowing for rapid diagnosis and treatment decisions. Similarly, in oncology, DWI helps differentiate between benign and malignant tumors based on their diffusion characteristics. Malignant tissues, with their higher cellular density, often exhibit restricted diffusion compared to benign lesions. This non-invasive approach eliminates the need for contrast agents in many cases, reducing risks associated with gadolinium-based dyes, particularly in patients with renal impairment.
Implementing DWI requires careful consideration of technical parameters to optimize image quality and diagnostic accuracy. The b-value, a measure of the strength and duration of the diffusion gradient, is a critical factor. Higher b-values increase sensitivity to diffusion but can degrade image signal-to-noise ratio. Clinicians typically use b-values ranging from 500 to 1000 s/mm² for most applications, balancing sensitivity and image quality. Additionally, the choice of diffusion directions (single vs. multiple) impacts the ability to detect anisotropic diffusion, as seen in white matter tracts. Advanced techniques like diffusion tensor imaging (DTI) build on DWI principles to map complex diffusion patterns, offering insights into tissue architecture and connectivity.
Despite its advantages, DWI is not without limitations. Motion artifacts, particularly in abdominal or cardiac imaging, can degrade image quality. Respiratory or cardiac gating techniques may be necessary to mitigate these effects. Interpretation also requires expertise, as certain conditions, such as T2 shine-through or perfusion effects, can confound diffusion measurements. For example, cysts or areas of vasogenic edema may falsely appear as restricted diffusion on DWI. Correlation with other MRI sequences and clinical context is essential for accurate diagnosis.
In practice, DWI has become an indispensable tool across multiple specialties. Neurologists use it to assess stroke, multiple sclerosis, and brain tumors, while radiologists rely on it for prostate, breast, and liver cancer evaluation. Its role extends to pediatric imaging, where it aids in diagnosing conditions like neonatal hypoxic-ischemic encephalopathy without exposing young patients to ionizing radiation. As technology advances, DWI continues to evolve, with emerging applications in functional imaging and treatment response monitoring, solidifying its place as a cornerstone of modern MRI.
Exploring Neodymium Magnets: Applications and Uses in Modern Technology
You may want to see also
Explore related products






![]()
Perfusion Imaging: Maps blood flow dynamics in tissues for functional analysis
Magnetic resonance imaging (MRI) leverages perfusion imaging to quantify blood flow dynamics within tissues, offering critical insights into organ function and disease progression. Unlike structural MRI, which captures static anatomy, perfusion imaging dynamically maps the delivery of blood to tissues, revealing how effectively cells receive oxygen and nutrients. This technique is particularly valuable in neurology, oncology, and cardiology, where understanding vascular health is essential for diagnosis and treatment planning.
To perform perfusion imaging, contrast agents such as gadolinium-based dyes are administered intravenously, typically at a dose of 0.1 mmol/kg, followed by a rapid saline flush to ensure optimal distribution. The MRI scanner then tracks the passage of these agents through the bloodstream, generating parametric maps that quantify parameters like cerebral blood flow (CBF), cerebral blood volume (CBV), and mean transit time (MTT). For example, in stroke assessment, reduced CBF and prolonged MTT in a specific brain region indicate ischemia, guiding thrombolytic therapy decisions. It’s crucial to monitor patients for gadolinium-related side effects, especially in those with renal impairment, as accumulation can lead to nephrogenic systemic fibrosis.
Perfusion imaging’s utility extends beyond acute conditions, playing a pivotal role in tumor characterization. In oncology, elevated CBV and CBF often correlate with angiogenesis, a hallmark of aggressive cancers. By comparing perfusion metrics before and after treatment, clinicians can assess therapy response earlier than with anatomical imaging alone. For instance, a 30% decrease in tumor CBF post-chemotherapy suggests effective anti-angiogenic activity. However, interpreting results requires caution, as factors like motion artifacts or inconsistent contrast injection can skew data. Standardizing protocols, such as using fixed injection rates (e.g., 5 mL/s) and breath-holding techniques, enhances reliability.
Pediatric applications of perfusion imaging demand special consideration. Children’s smaller vessels and higher heart rates necessitate tailored protocols, often employing lower contrast doses (0.05 mmol/kg) and age-specific scan parameters. Sedation may be required for younger patients to minimize motion, though this adds complexity to the procedure. Despite these challenges, perfusion MRI remains invaluable in diagnosing conditions like Moya-Moya disease, where abnormal collateral blood vessels form in response to arterial stenosis. Early detection through perfusion mapping can prevent stroke and guide surgical revascularization.
In summary, perfusion imaging transforms MRI from a structural tool into a functional one, enabling precise evaluation of tissue viability and vascular health. Its clinical impact spans from emergency stroke care to long-term cancer monitoring, with ongoing advancements in contrast agents and post-processing algorithms promising even greater utility. However, success hinges on meticulous technique, patient-specific adjustments, and awareness of potential pitfalls. By mastering these elements, clinicians can harness perfusion imaging’s full potential to improve diagnostic accuracy and patient outcomes.
Mastering Lead Magnets: Strategies to Attract and Convert Prospects Effectively
You may want to see also
Explore related products






![]()
Magnetization Transfer: Highlights macromolecular tissue components for detailed contrast
Magnetization Transfer (MT) is a specialized MRI technique that leverages the interaction between free water protons and macromolecular protons to enhance tissue contrast. Unlike conventional MRI, which primarily detects signals from free water, MT selectively highlights the bound water molecules associated with macromolecular structures like proteins, lipids, and glycosaminoglycans. This distinction allows MT to provide detailed insights into tissue microstructure, making it particularly valuable in neuroimaging, musculoskeletal imaging, and oncology.
To implement MT, a specific pulse sequence is applied, typically involving an off-resonance radiofrequency pulse that saturates the macromolecular protons. The degree of signal reduction in the resulting images reflects the concentration and mobility of these macromolecules. For example, in brain imaging, MT can differentiate between gray and white matter by emphasizing myelin content, while in cartilage imaging, it can assess proteoglycan integrity. Practical considerations include optimizing the off-resonance frequency (commonly 1-3 kHz) and pulse power to maximize contrast without causing excessive signal loss.
One of the key advantages of MT is its ability to detect subtle changes in tissue composition before they become apparent on conventional MRI. For instance, in multiple sclerosis, MT can reveal early demyelination by highlighting reduced myelin density in white matter lesions. Similarly, in osteoarthritis, MT can quantify cartilage degradation by mapping proteoglycan loss, often preceding morphological changes visible on standard MRI. This sensitivity makes MT a powerful tool for early diagnosis and monitoring disease progression.
However, MT is not without limitations. The technique is sensitive to magnetic field inhomogeneity, requiring careful shimming to ensure accurate results. Additionally, the interpretation of MT contrast can be complex, as it depends on both macromolecular content and water exchange rates. Clinicians and radiologists must therefore correlate MT findings with other imaging modalities and clinical data to avoid misinterpretation. Despite these challenges, MT remains a unique and valuable addition to the MRI toolkit, offering unparalleled insights into tissue microstructure.
Incorporating MT into routine clinical practice requires standardized protocols and specialized training. For example, in neuroimaging, a common MT ratio (MTR) calculation involves acquiring images with and without the off-resonance pulse and computing the signal difference as a percentage. Protocols should specify parameters such as flip angle (e.g., 500-1000 Hz), pulse duration (e.g., 50 ms), and repetition time (e.g., 500-1000 ms) to ensure reproducibility. As MT continues to evolve, ongoing research aims to simplify its application and expand its utility across diverse clinical scenarios, cementing its role in advanced tissue mapping.
Exploring Magnetic Resonance Imaging: Uses and Applications in Modern Medicine
You may want to see also
Frequently asked questions
Contrast agents, such as gadolinium-based compounds, are commonly used in MRI to enhance the visibility of specific tissues and improve diagnostic accuracy.
These substances alter the relaxation times of tissues, affecting how they appear on MRI images, which helps in distinguishing between different types of tissues and identifying abnormalities.
While generally safe, gadolinium-based contrast agents can pose risks to patients with kidney disease, as they may lead to a rare condition called nephrogenic systemic fibrosis. Proper screening is essential before administration.